DOI: S0100-72032015000400164 - volume 37 - Abril 2015
Joana Zanotti, Edison Capp, Maria Celeste Osório Wender
Excess weight is an increasing problem and a known risk factor for a number of chronic conditions, such as type 2 diabetes, dyslipidemia, and cardiovascular diseases, and its presence increases morbidity and mortality exponentially1 , 2. In women, excess weight is associated with an important moment in the life cycle: pregnancy. Retention of the weight gained during pregnancy may represent a determining factor for obesity and its development is the result of a complex network of factors3.
Average postpartum weight retention ranges from 0.5 to 3 kg among different populations4. In some studies, up to 20% of women have retained at least 5 kg from 6 to 18 months after delivery4. A study conducted in Rio de Janeiro, Brazil, showed that the average retained weight 9 months after delivery was 3.1 kg5. Greater weight retention was observed among women who were over 30 years old and had a pre-pregnancy body fat percentage of 30% or more5.
Excessive weight gain during pregnancy is the primary factor for postpartum weight retention4 , 6. Other factors associated with an increased risk of greater weight retention are high pre-pregnancy body mass index (BMI), short breastfeeding period, primiparity, smoking cessation, high calorie intake, and low physical activity, although these associations have not been found in all studies. A few studies7 , 8have evaluated the influence of diet and physical activity on postpartum weight change. Increased calorie intake and insufficient physical activity are associated with higher weight retention in some7, but not all8, studies. Some research has also associated weight retention with age8, marital status, and race9.
Psychological factors may also play a role in postpartum weight retention. It is known that psychiatric symptoms are common after delivery, a period marked by hormonal changes, as well as changes of a social nature and shifts in family organization, and by a high frequency of postpartum depression10. Sleep disorders and depression also seem to be associated with postpartum weight retention11 , 12. It has been demonstrated that early (three and six months) postpartum body image dissatisfaction is related with postpartum weight retention at nine months13.
Even though scientific literature about this subject is growing, the factors of postpartum weight retention have yet to be explored in different settings and populations. The aim of this study was to analyze the association between predictive factors and postpartum weight retention after six months.
This study is a cohort analysis of data collected on day one and one, three, and six months after delivery. The sample comprised women who delivered from September 2010 to April 2011. Participants were invited to take part and were enrolled after providing written Informed Consent. The institutional review board of Hospital do Círculo, Caxias do Sul, Brazil, approved the study protocol (CEP Círculo-FSG #0094). Data was collected on the first day after childbirth and during hospitalization.
Puerperal women between the ages of 19 and 45 years and with a gestational age of 38 to 42 weeks were recruited from the maternity service of Hospital do Círculo, a hospital located in Caxias do Sul, a city in Southern Brazil (population: 450,000). Twin pregnancies, patients with physical limitations precluding anthropometric measurement, patients with conditions that could cause changes in body weight (diabetes mellitus, hypertension, thyroid disease) or psychiatric disorders, and women who missed at least one study visit were excluded from analysis.
At the start of the study, 219 mothers were enrolled. At 6-month follow-up, 74 patients (33.8%) of the sample had been lost: 61 did not return to the scheduled appointments, 11 could not be found and 2 moved from the city. Failure to attend study visits and inability to contact the patient were the main reasons for the loss of the follow-up.
Socioeconomic profile (educational attainment, family income, and marital status) was assessed by means of a specific questionnaire during the first study interview, as well as relevant biological profile was included along with reproductive factors (skin color, age, parity, inter-pregnancy interval, and mode of delivery).
Dietary intake was assessed at the 1-month, 3-month, and 6-month postpartum visits by means of a 24-hour food recall (to quantify calorie, carbohydrate, protein, and lipid intake) and a validated food frequency questionnaire14. Quantities were estimated in household measurements for a typical day. The DietWin Professional 2.0 software suite was used to calculate calorie, macro and micronutrient intake.
Adequacy of calorie intake was analyzed by comparison with the recommended daily allowance (RDA) standard15. For women between the ages of 19 and 45, an intake of 2,200 calories a day, plus an additional intake of 500 calories for the puerperal period, was considered adequate.
Adequacy of macronutrient intake (carbohydrates, proteins and lipids) was calculated on the basis of Dietary Reference Intakes (DRIs)16. Current DRIs recommend that, in postpartum women aged 19 to 45 years, carbohydrates account for 45 to 65%, proteins for 10 to 35%, and lipids for 20 to 35% of total calorie intake, respectively16.
The anthropometric variables of interest were pre-pregnancy weight and weight preceding delivery, both self-reported by the participant. Weight was measured at every study visit and height only once, during the second visit. Both parameters were measured by the same investigator, using standard anthropometric techniques. Pre-pregnancy BMI and total weight gain during pregnancy were classified according to the World Health Organization (WHO)2 and the Brazilian Ministry of Health17recommendations, respectively.
Data on physical activity were collected with the International Physical Activity Questionnaire (IPAC)1, which was administered during the post-delivery study visits. The Beck Depression Inventory (BDI) was used to assess depression18. All questionnaires have previously been validated to Portuguese19.
Sample size was calculated with the PEPI 4.0 software. For a significance level of 5%, a statistical power of 85%, and a minimum effect size of 0.3, the minimum sample size was 148 postpartum women5. Initially, 219 patients were enrolled, anticipating potential losses. Data analysis was performed using Statistical Package for the Social Sciences (SPSS) 17.0 software. Quantitative variables were described as mean ± standard deviation, and the categorical variables, through absolute and relative frequencies. Student's t-test or one-way analysis of variance (ANOVA) followed by Tukey's test were used to compare means. Correlations were assessed with Pearson's and Spearman's tests, as indicated. To identify and evaluate confounders independently associated with total weight loss, a multivariate linear regression analysis was performed. The statistical significance level was set at p≤0.05.
The sample consisted of 145 women, with a mean age of 25±6 years (range, 19-45 years). Pre-pregnancy weight was 65±13 kg and pre-pregnancy BMI, 23.9 (±4.7) kg/m². Most participants had studied for more than 8 years (86.2%), were married (87.6%), white (86.2%), and primiparous (66.2%). Among the 49 women who had previous children, 73.5% had become pregnant after an interval of at least 2 years. On further analysis of parity, 39 participants (26.9%) had 2 or 3 children and 10 (6.9%) had 3 or more children. Regarding socioeconomic status, 67 (46.2%) had a household income Brazilian minimum wages, 69 (47.6%) over 5 minimum wages, and only 9 (6.2%) earned less than 2 minimum wages. The mean (standard deviation - SD) number of persons dependent on the household income was four. The vast majority of participants delivered by cesarean section (93.8%) and were nonsmokers (94.5%). Table 1 describes the sample profile in further detail.
Table 1 -
Sample profile
| n | |
|---|---|
| Educational attainment (years) | |
| <8 | 20 |
| >8 | 125 |
| Skin color | |
| White | 125 |
| Brown | 15 |
| Black | 5 |
| Parity | |
| Primiparous | 96 |
| 2–3 children | 39 |
| >3 children | 10 |
| Mode of delivery | |
| Cesarean section | 136 |
| Vaginal | 9 |
| Marital status | |
| Single | 18 |
| Married | 127 |
| Family income | |
| <2x minimum wage | 9 |
| 2–5x minimum wage | 67 |
| >5x minimum wage | 69 |
| Smoking | |
| Non-smokers | 137 |
| Smokers | 8 |
| Maternity leave (months) | |
| <4 | 33 |
| >4 | 112 |
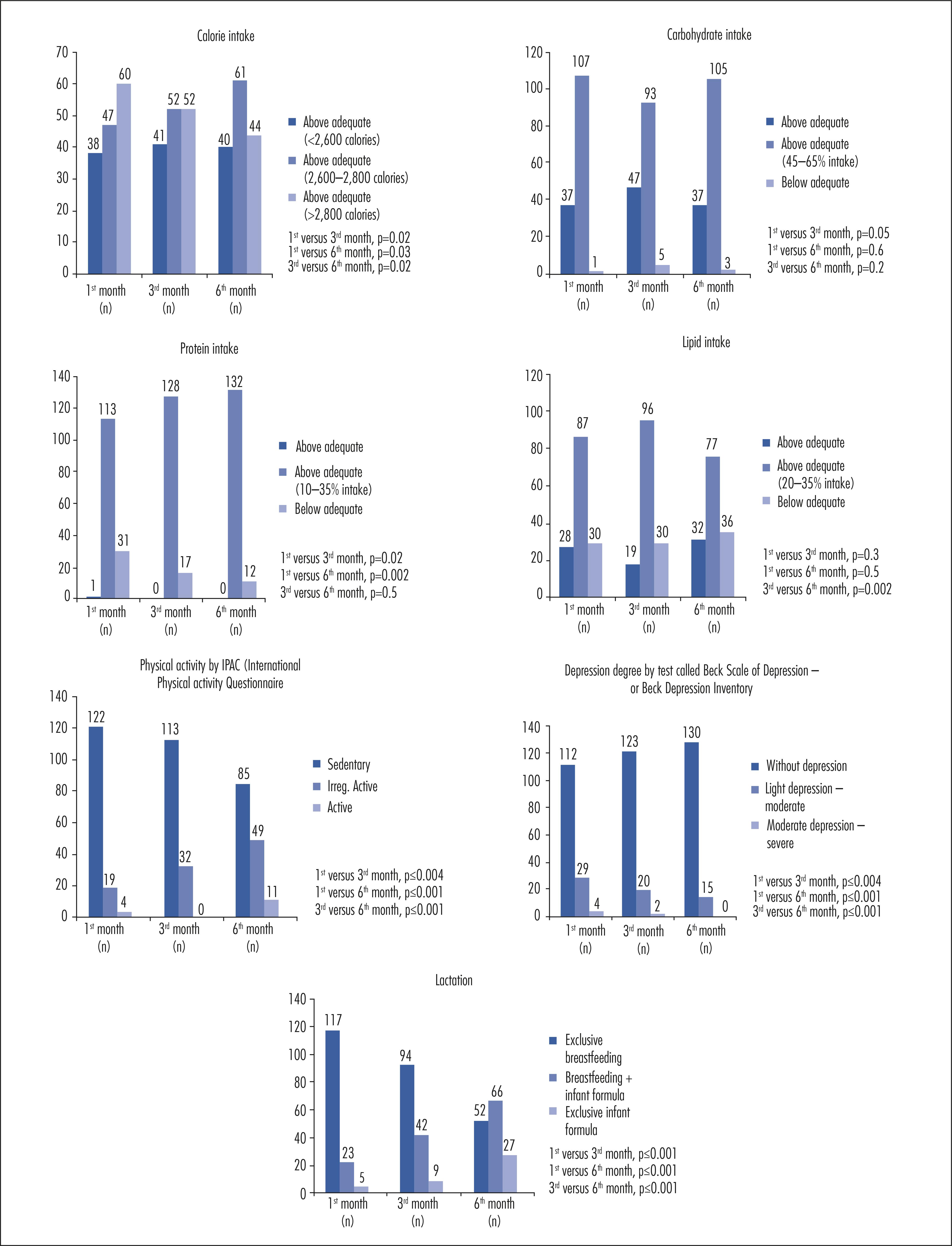
Figure 1 provides data on macronutrient intake, physical activity, depression (as assessed by the BDI), and lactation. Comparison of macronutrient intake over the six-month study period showed a statistically significant difference in calorie intake between the sixth month and the other months; the proportion of women reporting adequate calorie intake increased significantly in the last month of the study.
Figure 1 -
Comparison of calorie intake, macronutrients, physical activity, depression, lactation.
Over the course of the study, the participants began to incorporate physical activity into their routines. There was a reduction in the number of women who had a sedentary lifestyle and an increase in the number of women who exercised. Analysis of the degree of depression over time showed an increase in the number of patients without depression during the study period. Conversely, the percentage of exclusive breastfeeding declined over the 6-month study period, to a nadir of 35.9% in the last month of the study (Figure 1).
Overall, mean (SD) weight loss from day 1 after delivery to month 6 of follow-up was 9.5±4.1 kg. The difference in weight over time was significant at all time points of analysis (p<0.001). The mean weight retention at the end of the 6-month study period was 4.8 kg.
When the quantitative variables of interest were tested for association with total weight loss, a significant positive association was found between total weight gain and physical activity during pregnancy. In other words, the greater the total weight gain (excluding adequate pre-pregnancy BMI) and the level of physical activity frequency during pregnancy, the greater the weight loss (i.e. lower weight retention). The average weight loss was found to be 68% of the total weight gained. For other associated parameters, the ratio was reversed: greater parity, inter-pregnancy interval, calorie intake, pre-pregnancy BMI, depression scores, and lack of exclusive breastfeeding were directly associated with lower weight loss, i.e.greater weight retention.
Concerning nominal variables, total weight loss was significantly associated with educational attainment and marital status. Women who had more than eight years of formal schooling and married women retained the least weight. There was no statistically significant association between skin color or mode of delivery and total weight loss.
Multivariate linear regression analysis was carried out to adjust for potential confounders. The variables that remained significantly associated with weight retention were calorie intake, pre-pregnancy BMI, lactation, and marital status. The women who retained the least weight were those who consumed fewer calories, had a lower BMI before pregnancy, did not experience excessive weight gain during pregnancy, breastfeed their babies exclusively for a longer period, and were married (Table 2).
Table 2 -
Variables independently associated with weight loss in postpartum women (multiple regression analyses, n=145)
| Variables | b | ß | p-value |
|---|---|---|---|
| Calorie intake | -0.953 | -0.189 | 0.008 |
| Pre-pregnancy BMI | -0.229 | -0.262 | 0.001 |
| Excessive weight gain | -4.20 | -0.412 | <0.001 |
| Exclusive breastfeeding | 1.60 | 0.153 | 0.045 |
| Married | 2.53 | 0.204 | 0.004 |
Multiple regression analyses variables: parity, inter-pregnancy interval, calorie intake; pre-pregnancy BMI, excessive weight gain, depression, exclusive breastfeeding, educational attainment >8 years, married. Variables with significant association are presented inTable 1. BMI: body mass index.
There was a significant difference between the total weight gain category and that of total weight loss. Women who gained excessive weight, as defined by pre-pregnancy BMI, were those who lost the least weight on average (pregnancy weight gain insufficient, 9.8±2.5 kg; adequate, 10.2±4.3 kg; excessive, 6.3±2.7 kg; p<0.001).
A significant association between pre-pregnancy BMI and depression was also observed (rš=0.344; p<0.001). In other words, patients with a higher BMI exhibited higher levels of depression. Furthermore, women who had less depression breastfed exclusively for longer periods (rš=0.489; p<0.001). The latter association held even when pre-pregnancy BMI was not taken into account (p=0.002).
In this study, the women who retained less weight postpartum were those who ingested less calories, who were married, those who did not experience excessive weight gain during pregnancy, those who breastfed exclusively during the first months after delivery, and who had a lower BMI prior to pregnancy. Similar to previous studies, pre-pregnancy, most of the patients were eutrophic20 , 21.
More years of education were associated with less postpartum weight retention. This is consistent with previous research, which found that women with low education are more likely to develop obesity22. Investigations conducted by Kac et al. revealed that women with difficulty or inability to read a letter were 2.1 times more likely to retain ≥7.5 kg, 9 months after delivery23. According to the literature, the higher the level of education, the lower the weight in the postpartum period. For each increment of 1 year of formal schooling, the weight is reduced by 1.3 kg. Women with more than five years of schooling have a clear tendency to lose weight until nine months after childbirth5.
In the present study, marital status was associated with postpartum weight retention. In general, married women had lower levels of weight retention at the end of the study. It has been previously suggested that single women have a higher risk of developing obesity, and unmarried women between the ages of 25 and 45 years old have greater weight retention associated with parity. Nevertheless, Gunderson et al. found no association between marital status and maternal obesity24.
The mean weight retention in multiparous and primiparous women was 49 and 24%, respectively, by the end of the 6-month study period. On average, primiparous women lost 76% of the weight gained during pregnancy versus 51% in multiparous women. Some studies had observed an association between associated parity and overweight. In a study of 2,338 Brazilian women, after the birth of their first child, the participants gained, on average, 0.9 kg per year up to 8 years after delivery, and the prevalence rates of overweight and obesity increased from 11.5 and 1.7% to 25.2 and 9.3%, respectively, after the first pregnancy25. Two other studies have also shown higher weight retention among multiparous as compared with primiparous women. Conversely, Dewey et al.26 found a negative association between parity and weight retention, although their sample size was small. Inconsistent findings regarding parity may be attributable to errors in the reporting of pre-pregnancy weight or failure to control for other characteristics associated with parity and weight gain27.
Of the women included, 49% exhibited weight gain above the recommended range during pregnancy, whereas 31 and 29% showed adequate and below-adequate weight gain according to pre-pregnancy BMI, respectively. Weight gain during pregnancy has been described as one of the most important determinants of weight retention during the postpartum period. In the present study, excessive weight gain during pregnancy was associated with higher weight retention, as in previous investigations28. Scholl et al.29 found that, at 6 months after delivery, women with excessive weight gain had retained 40% of the gained weight and were 12% heavier than they were before pregnancy.
Postpartum weight retention is an important nutritional problem for women of childbearing age30, especially in Brazil, where 47.4% of women are overweight and 17.5% are obese31. Women with gestational weight gain above the upper limit have twice the probability of retaining 9 kg postpartum compared with women with recommended weight gain32. Longitudinal studies have shown a relationship between gestational weight gain and subsequent maternal obesity and indicated that gestational weight gain along with weight retention at one year postpartum is associated with long-term obesity32 - 34.
The influence of breastfeeding on weight in the postpartum period is controversial. As it has been demonstrated previously35 , 36, in the present study, weight retention was lower in women who breastfed exclusively for a longer period. Breastfeeding seems to have a protective effect against weight retention. Women who breastfed their children for longer (whether exclusively or mixed feeding) or had higher lactation scores tended to lose more weight between 2.5 and 12 months after delivery. Dewey et al.26 analyzed patterns of weight loss over a 24-month period after childbirth and found that, at 6 months after delivery, the average weight among mothers who breastfed was approximately 2.8 kg lower than that of women who had breastfed for less than 3 months, in a cohort study with 5-year follow-up they found that the association between breastfeeding and weight change was complex and, in their sample, weak. Kramer et al.37, in turn, studied 411 women and did not find any association between breastfeeding and postpartum weight loss.
One interesting finding of our study is the negative association observed between depression scores (as measured by the BDI) and breastfeeding, as well as the positive association between depression scores with BMI and with weight retention. Similarly, Herring et al.38 showed that women who experienced postpartum depression were more than twice as likely to retain at least 5 kg in a 1-year period after delivery. Another study conducted with 25 low-income women showed that depressive symptoms in the postpartum period were associated with greater weight retention in this period39. Recently, a systematic review showed that a research investigating the impact of postpartum sleep, stress, depression on weight retention is limited and future longitudinal studies are needed40. Whitaker et al.12 found a significant association between stress and weight retention. Phillips et al.13 showed that weight gain during pregnancy, breast feeding (six or less months), body image dissatisfaction in months three and six after delivery were associated with more postpartum weight retention.
This study used data about pre-gestational weight as self-reported by the patients, which may lead to an estimation bias. However, previous studies have shown a high positive correlation between reported and measured pre-gestational weight41.
The follow-up in the present study was six months and a non-population-specific questionnaire was used to quantify daily dietary intake. Unfortunately, at 6-month follow-up, 33.8% of the patients did not return to their appointments. These may also be considered limitations of this study.
Maternal age, income, number of dependents, and physical activity after delivery were associated with greater weight retention. Regarding the influence of pre-existing factors on weight change during the postpartum period, pre-pregnancy nutritional status, physical activity during pregnancy, weight gain adequacy and lower parity were most influential. Breastfeeding, food intake, and level of depression were also determinants of postpartum weight variation. Excessive maternal weight gain during pregnancy must receive special attention during prenatal care due to its association with postpartum weight retention. Nutritional and physical activity interventions should be taken during pregnancy as well as postpartum in order to prevent weight retention. It is worth noting that there is still a dearth of research into postpartum weight retention and depression, which suggests a need for further studies on the subject.